The content on this web page was written by Dr. med. Julien Billières.
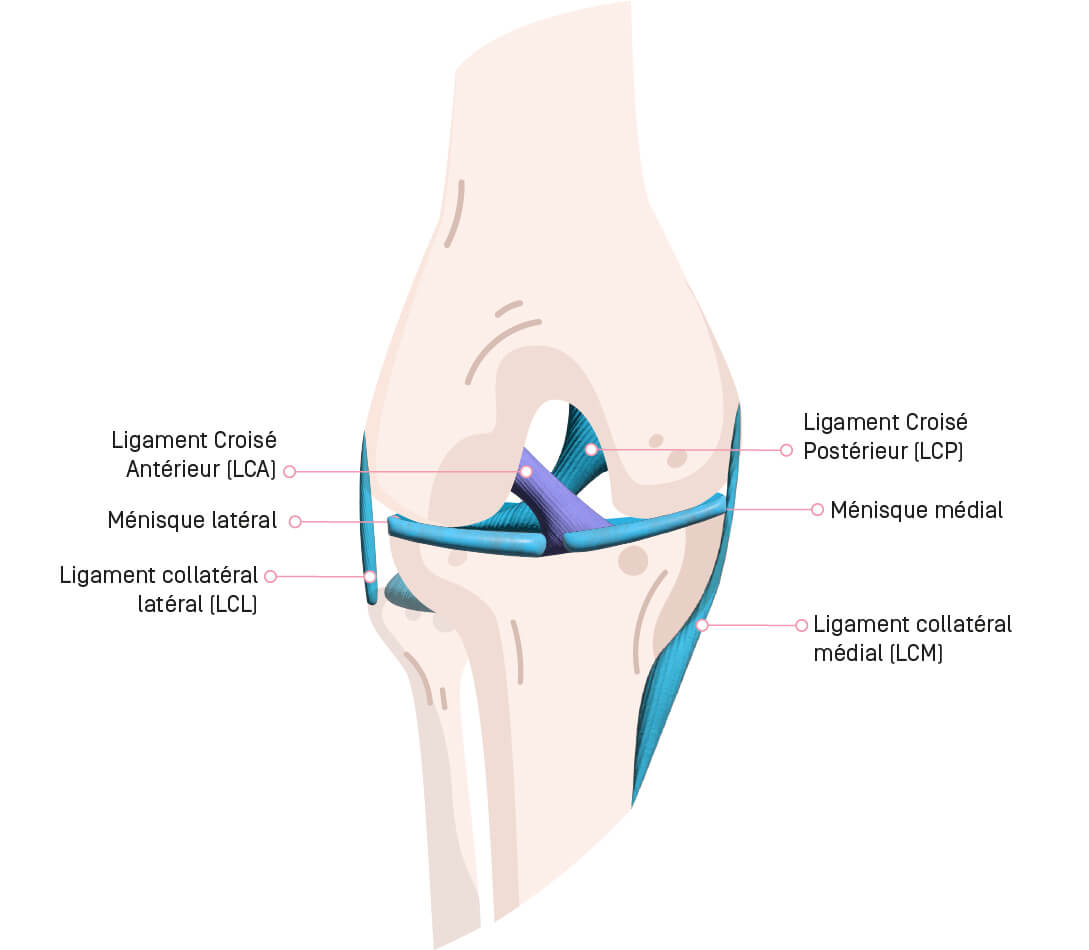
The knee joint consists of the femur, the tibia, and the patella. It is stabilized by these four main ligaments:
- the anterior cruciate ligament (ACL),
- the posterior cruciate ligament (PCL),
- the medial collateral ligament (MCL),
- and the lateral collateral ligament (LCL).
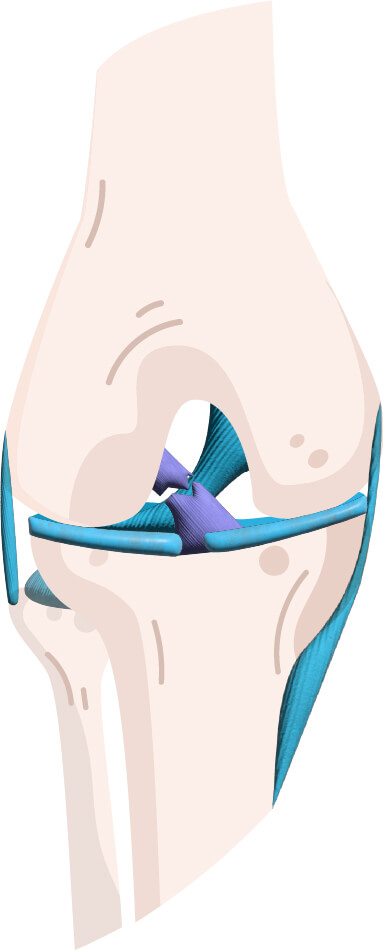
The ACL is crucial for knee stability; it prevents the tibia from shifting forward and rotating inward relative to the femur. Most ACL tears occur in people who participate in sports involving changes in direction, such as soccer, basketball, and skiing. The tear is rarely partial; more often than not, it is complete or nearly complete. It is frequently accompanied by meniscal tears (~30%), a tear of the anterolateral ligament (~90%), or a tear of the medial collateral ligament (~30%). Depending on the type of tear and the associated injuries, healing of the ACL may not be possible. You may then experience varying degrees of knee instability, ranging from difficulty resuming sports activities to discomfort in daily life with episodes of the knee giving way or buckling. In the short and medium term, this laxity leads to new meniscal injuries or worsens existing ones. In the long term, this can lead to early-onset osteoarthritis.
Functional treatment involving physical therapy and follow-up care from a sports medicine specialist is recommended in cases of mild laxity, provided there are no significant meniscal tears and/or high-risk activities.
Anterior Cruciate Ligament Reconstruction
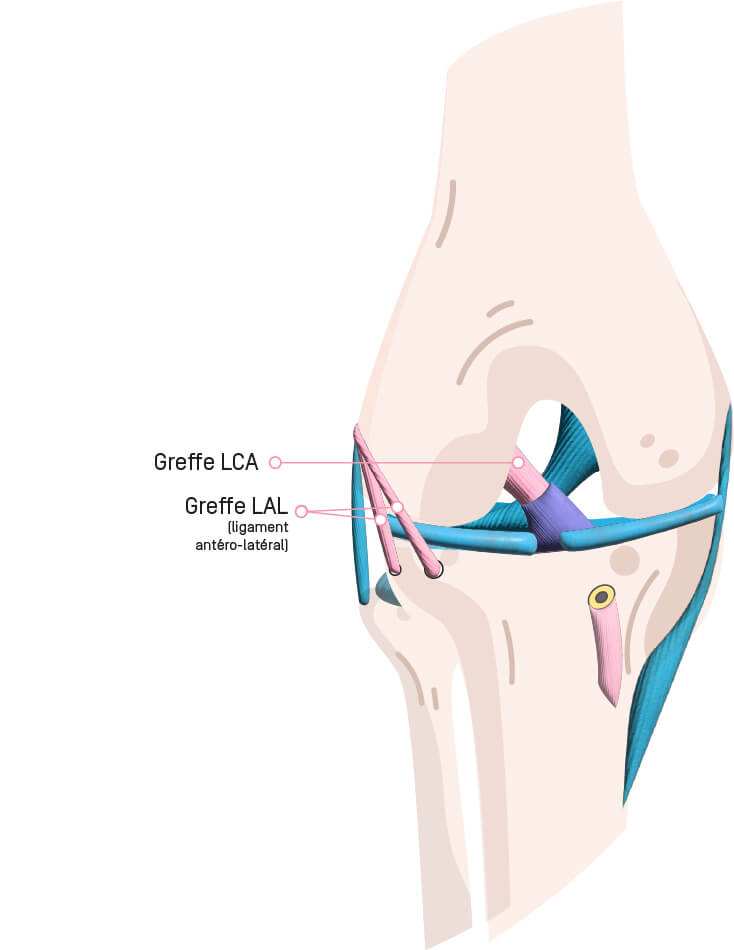
The surgical treatment of choice is ACL reconstruction, or ligamentoplasty, to stabilize the knee. It is performed arthroscopically under general anesthesia or spinal anesthesia. To reconstruct this ligament, a section of tendon from around the knee must be harvested. The three most common options, which yield the best results, are: the patellar tendon, the quadriceps tendon, or the hamstring tendons (DIDT). These three types of grafts produce equivalent results. A portion of these tendons is harvested using a minimally invasive technique (resulting in a small scar). The use of an allograft (tendon from a donor) is not recommended due to the higher risk of rupture. Tunnels are created in the tibia and femur, and the graft is threaded through them to anatomically reconstruct the ACL. It is then secured within the bone using resorbable screws.
During this surgery, using arthroscopy, your surgeon will evaluate the menisci and cartilage. If any damage is found, the surgeon will perform the necessary treatment (such as repairing a torn meniscus). During the same surgical procedure, the anterolateral ligament (ALL) of the knee can also be reconstructed using a minimally invasive technique. This additional procedure helps better control knee rotation and reduces the risk of a new anterior cruciate ligament tear and meniscus suture failure.
The surgery lasts between 30 and 60 minutes, depending on whether meniscal tears need to be repaired.
In some more severe cases, it may be necessary to repair or reconstruct one of the collateral ligaments and to wear a knee brace afterward.
After the surgery
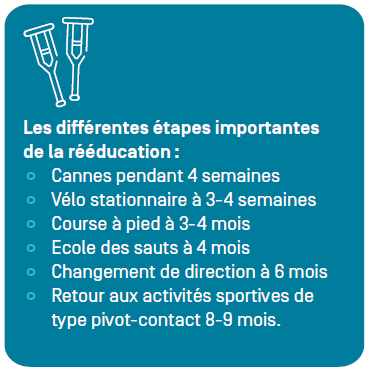
You will stay in the hospital for 2 to 4 nights. A physical therapist will visit your room twice a day to teach you how to walk with crutches and show you the exercises to do at home. A splint is not necessary, and you will walk with full weight-bearing support using crutches for 4 weeks. Some meniscal repairs require partial weight-bearing with canes for 6 weeks. The knee will be swollen for the first 2–3 weeks, and a bruise may develop. You should apply ice to your knee frequently (every two hours).
On the way out
You will receive: a prescription for medication, a medical certificate, appointment schedules for dressing changes and follow-up visits with your surgeon, physical therapy vouchers, and the rehabilitation protocol. Physical therapy begins 7 to 10 days after surgery, at a rate of 2 to 3 times per week. It is best to schedule in advance your appointments as soon as your surgery date is known.
Postoperative follow-up is conducted jointly by your surgeon and a sports medicine physician at Hôpital de La Tour to optimize your rehabilitation. Follow-up appointments take place every 1 or 2 months until you are ready to return to sports. Your commitment to rehabilitation is crucial and ensures a successful surgical outcome. To this end, your physical therapist, surgeon, and sports medicine physician will provide you with the necessary instructions to regain your mobility, strength, endurance, and balance. Starting 6 months after surgery, your sports medicine physician will conduct isokinetic and functional tests at the La Tour rehabilitation center. The goal is to objectively assess the strength and neuromuscular control of the lower limb using tests validated in the scientific literature. Depending on the results, a return to sports activities will either be permitted or postponed. A return to pivot-contact sports (soccer, basketball, skiing, etc.) is generally permitted starting at 8–9 months.
Is the surgery urgent?
No, in most cases, this surgery is scheduled within weeks of the injury, but no later than 6 months (due to an increased risk of secondary meniscal tears). Sometimes it is even necessary to wait for the swelling in the knee to subside and for the quadriceps muscle to regain strength through preoperative physical therapy sessions. However, depending on the type of meniscal tear (bucket-handle tear, complete radial tear) and/or in the event of a complete collateral ligament tear, surgery must be performed promptly to achieve the best outcome.
What are the complications?
Complications are uncommon:
- Infection (rare),
- hemarthrosis (rare),
- venous thrombosis (rare),
- joint stiffness (~1–2% of cases requiring reoperation),
- recurrent ACL tear (risk no higher than on the opposite side),
- failure of a repaired meniscus to heal (up to 10% depending on the extent of the injury to be repaired),
- loss of sensation around the scars.
Everything You Need to Know About an Anterior Cruciate Ligament Tear
To learn more about anterior cruciate ligament tears, watch our public lecture featuring our expert, Dr. Julien Billières, by clicking here
Find Us
Contact
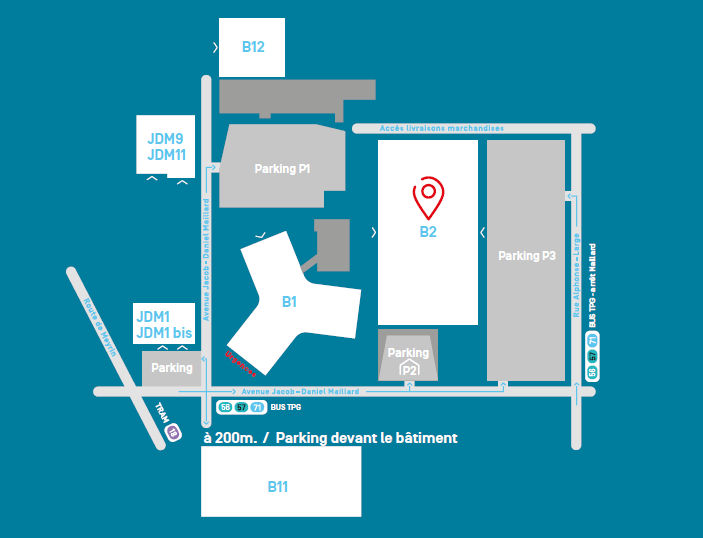
Hôpital de la Tour - Bâtiment B2
Avenue J.-D. Maillard 3
1217 Meyrin
+41 (0) 22 719 66 40
cabinet.billieres@latour.ch
Le plan de situation
Knee Surgery
FMH Orthopedic Surgery and
Traumatology of the Musculoskeletal System
Sports Medicine SSMS