This is a chronic condition that can significantly affect quality of life due to the pain, difficulty walking, and discomfort when wearing shoes that it causes. Over time, this deformity can become rigid, causing painful skin lesions.
Symptoms of hammer toes
Symptoms vary depending on the stage of progression of the deformity. Hammer toes most often mani-fest as discomfort in shoes. The toe bends abnormally, causing constant rubbing against the top of the shoe. This friction can lead to the development of corns or calluses (painful thickening of the skin), often at the middle joint of the toe or at its tip.
At first, the deformity remains flexible: the toe can be straightened with the fingers. But over time, the toe becomes fixed in a bent position, making movement more difficult and increasing pain. This pain is mainly felt when walking, putting on shoes, or after prolonged exertion.
In advanced cases, the toe presses abnormally on the ground with its tip, which can cause significant pain under the foot (metatarsalgia). Redness, swelling, or difficulty stretching or bending the toe completely may also be observed.
In people with diabetes, these lesions can develop into sores or infections and therefore require special attention
Causes of hammer toes
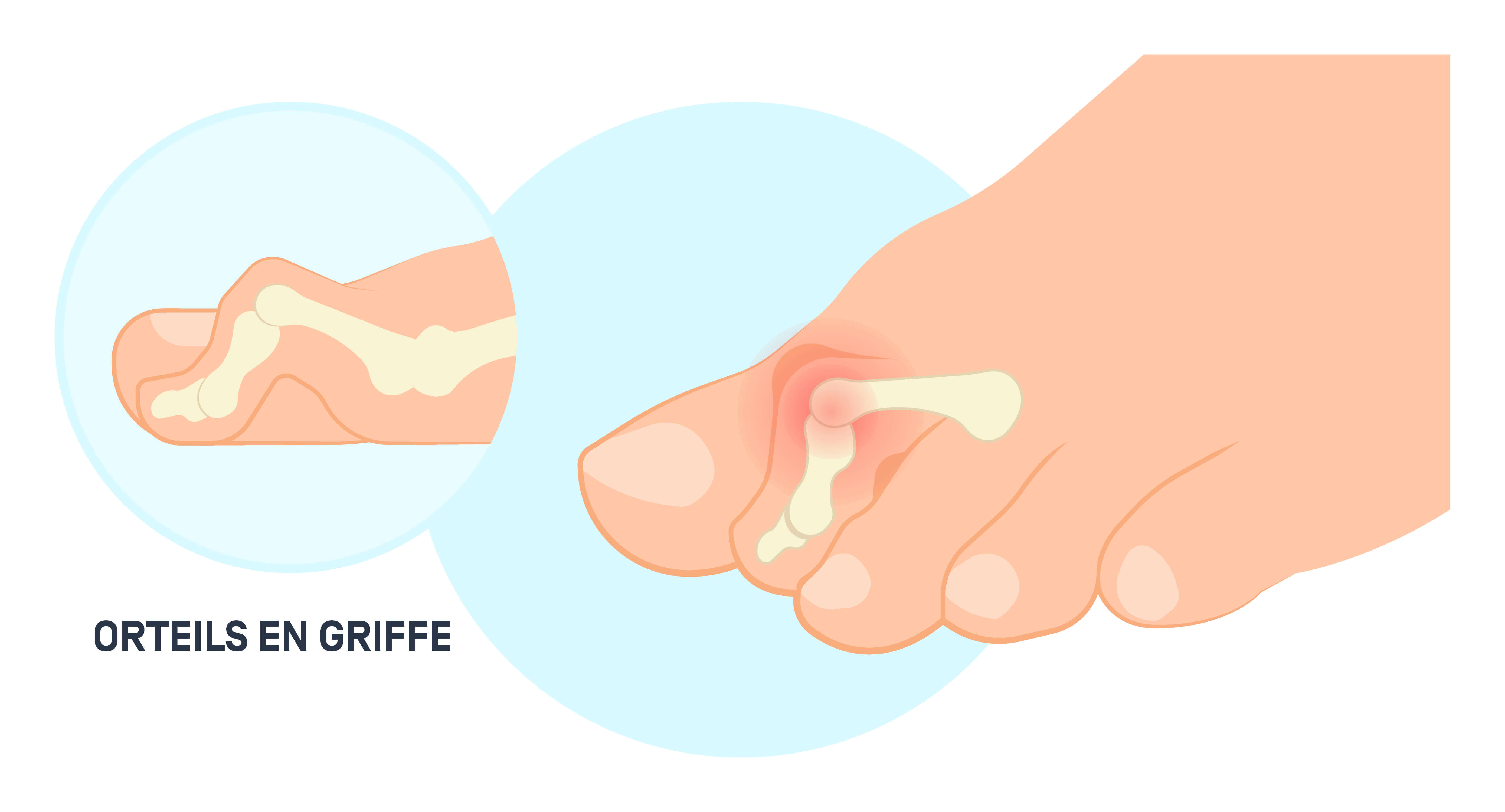
Hammer toe deformity results from a muscular imbalance between the powerful extrinsic muscles and the weaker intrinsic muscles of the foot. This imbalance alters the harmony of the forces exerted on the digital joints, promoting flexion of the phalanges and extension of the metatarsophalangeal joint. This mechanism is often triggered or aggravated by mechanical factors such as wearing narrow, rigid, or high-heeled shoes, which force the toes into an abnormal and prolonged position.
Associated conditions such as hallux valgus, high arches, or certain chronic neurological or inflammatory diseases can contribute to the onset of this deformity. The shape of the foot, particularly the “Greek foot” morphology (with a second toe longer than the first), also increases the risk.
Risk factors of hammer toes
Some people are more prone to developing hammer toes due to anatomical characteristics, associated conditions, or lifestyle factors. Being female is a recognized predisposing factor. Women are more often affected by this condition, probably due to the frequent wearing of narrow shoes or high heels, which increase mechanical stress on the toes. Shortening of the first metatarsal bone (index minus), flat feet, or associated deformities, particularly hallux valgus, significantly increase the risk.
Age is also a determining factor, with the risk increasing after the age of 50. Family history seems to play a significant role, as does the presence of systemic conditions such as rheumatoid arthritis or diabetes, which alter neuromuscular function or joint integrity. Finally, certain foot shapes, such as high arches or Greek feet, expose the forefoot to an imbalance of forces, thereby promoting deformity.
Diagnosing hammer toes
The diagnosis of claw toes is based primarily on clinical examination, which allows the affected joints to be identified and the flexibility of the deformity to be assessed. Observation under load (standing) and without load (sitting or lying down) is essential to distinguish between flexible forms, which can be manually reduced, and rigid forms.
The doctor also inspects the skin, looking for corns, calluses, redness, or lesions. Palpation of the foot, particularly at the base of the toes, allows for the evaluation of possible pain in the metatarsophalangeal joint, often associated with joint instability. This can be confirmed by the modified Lachman test, which involves moving the toe upward to detect subluxation or laxity.
Imaging completes the assessment: a weight-bearing X-ray of the foot allows visualization of joint alignment and detection of dislocation, osteoarthritis, or bone deformities. In some cases, ultrasound may be useful for visualizing tendon structures or the plantar fascia.
Treating hammer toes
Treatment depends mainly on the stage of the deformity and the level of discomfort experienced. In early stages and when the deformity is still flexible, conservative treatment is preferred. This involves wearing suitable shoes that are wide at the front, with flexible soles and no excessive heel. Foot orthotics or silicone orthotics can also relieve painful pressure points and partially correct the toe's posture.
Regular care from a podiatrist, particularly to remove corns or calluses, can help to alleviate pain. At the same time, rehabilitation exercises, such as picking up small objects with the toes or “towel curls,” can strengthen the intrinsic muscles of the foot and slow the progression of the deformity.
When the pain becomes debilitating or the deformity is rigid, surgery may be recommended. The most common technique is arthrodesis of the proximal interphalangeal joint, which involves removing the cartilage and immobilizing the joint with a temporary pin. Today, minimally invasive alternatives, known as percutaneous techniques, allow for effective correction with very limited incisions and often without the need for implanted material. Thanks to minimal tissue trauma, recovery is faster.
Progression and possible complications
The natural progression of hammer toes is marked by a gradual worsening of symptoms. What starts as simple discomfort when walking or wearing shoes can, if left untreated, lead to irreversible and painful deformity.
In the initial stage, the deformity is said to be reducible: the toe can be manually returned to its natural position. But over time, the shortened tendons lose their elasticity, the joints stiffen, and the claw becomes rigid. At this stage, the pain intensifies, and corns, hyperkeratosis, or sores frequently develop. If these skin lesions are not properly monitored, particularly in people with diabetes, they can develop into ulcers or severe infections.
The most feared joint complication is metatarsophalangeal dislocation, which occurs when the toe is completely displaced from its axis. This situation causes major mechanical instability, resulting in intense metatarsalgia due to overload on the corresponding metatarsal head.
When should you contact the Doctor?
Medical consultation is necessary as soon as pain appears in the toes or persistent discomfort when walking or wearing shoes. A toe that begins to bend abnormally, accompanied by redness, painful calluses, or difficulty fully extending the toe, should be cause for concern.
In people with diabetes, even the slightest change in the appearance of the skin or joints of the toes (wounds, ulcers, rubbing) requires prompt evaluation. This follow-up is essential to prevent infectious complications, which are common and sometimes serious in this context.
Progressive toe stiffness, intense plantar pain, or visible deformity are also indications for specialized care, including surgery if conservative treatments are ineffective.
Care at Hôpital de La Tour
At Hôpital de La Tour, hammer toes are treated by a team specializing in foot surgery, working closely with the physiotherapy and podiatry departments. Each patient receives a comprehensive assessment and personalized treatment tailored to their level of discomfort and goals.
The hospital has state-of-the-art equipment for diagnosis and minimally invasive surgery, including percutaneous surgery, which allows for rapid recovery with minimal discomfort. Support continues after the procedure with tailored care, targeted rehabilitation, and attentive follow-up
FAQ on hammer toes
Can hammer toes correct themselves naturally?
In the early stages, when they are still flexible, certain measures such as wearing appropriate shoes, exercises, and orthotics can slow down the progression, but complete spontaneous correction remains rare.
Should high heels be avoided?
Yes. High heels increase pressure on the forefoot, promote metatarsophalangeal extension and flexion of other joints, thereby accelerating the formation of hammer toes.
Can you continue to exercise with hammer toes?
Yes, but certain adjustments are necessary. A specialist can recommend suitable footwear and orthotics to limit pain during exercise.
Is surgery always necessary?
No. Only rigid or very painful forms that are not relieved by conservative treatments warrant surgery.
How long does it take to recover after surgery?
It varies depending on the technique used. With percutaneous surgery, it is often possible to return to wearing normal shoes after 2 to 3 weeks, compared to 6 to 8 weeks with open surgery.
Is surgery painful?
Modern minimally invasive techniques significantly reduce post-operative pain and speed up recovery. Effective pain management is always provided.
Can claw toes be prevented with exercises?
Mobilization and muscle strengthening exercises can help maintain the functional balance of the foot, especially as a preventive measure or at the first signs of deformity.