Dr. Faundez, what was the patient’s condition?
The patient was suffering from lumbar sciatica caused by a herniated disc. To put it simply, in these situations, part of an intervertebral disc protrudes into the lumbar spinal canal and compresses a nerve—often the sciatic nerve, as in this specific case. This results in lower back pain that follows the nerve’s path—in this patient’s case, extending down into the left leg. It is one of the most common back conditions, caused by natural aging, and surgery is performed when there is significant weakness or when the pain persists for too long.
How is this procedure typically performed?
The standard technique for a herniated disc is microdiscectomy, which involves removing the herniated portion under a microscope. The procedure is performed through a small incision, the size of which may vary depending on the patient’s profile and body type.
This technique works very well, but it has one drawback: it involves detaching the muscles, which causes slight damage and, more importantly, leads to lower back pain for a few weeks. Although this is not insurmountable, it limits activities and prolonged standing or sitting and increases the need for pain medication.
In short, it eliminates the initial sciatic pain, but with the drawback of temporarily causing post-surgical lower back pain.
Does the endoscopic technique help avoid this?
The endoscopic technique improves recovery. However, it has struggled to gain traction in Europe, mainly because a technique called “monoportal” had been used until then. This involves inserting a single tube that passes through the musculature without damaging it to reach the herniated disc. The main problem with this technique—which has largely prevented its widespread adoption—is its complexity: it requires extensive practice to become proficient, which is why few surgeons have adopted it.
What innovation finally made it more accessible?
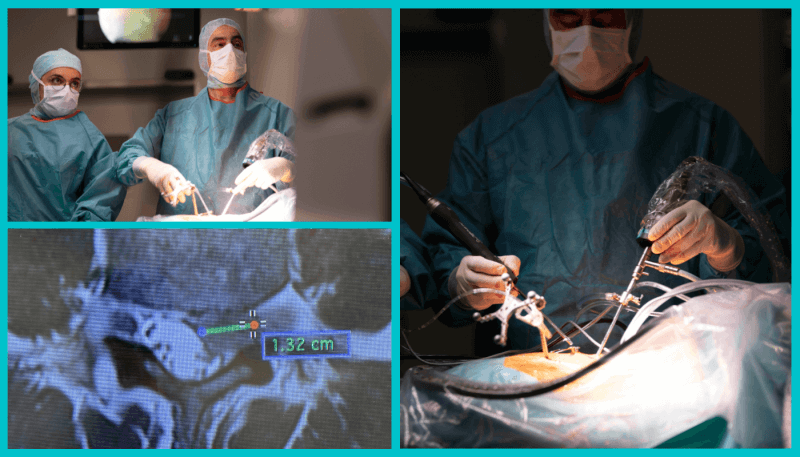
What we performed a few days ago was a first in French-speaking Switzerland and the second in Switzerland—a procedure still rarely performed in Europe. However, this procedure is not new and has already proven effective in Asia—particularly in South Korea—for several years. With this technique, known as the biportal technique, we use two access points instead of one, which provides a better working field.
We make an incision for the instruments, which passes through the muscle tissue with minimal damage, and through which we remove the hernia. At the same time, a second incision is made for the camera, giving us complete visual control. The working angle is therefore better, whereas with the monoportal technique, all the instruments are in the same field of view, which makes the procedure more complex.
Beyond the benefits for the patient, is this a real advantage for the surgeon?
Absolutely. For orthopedic surgeons who are already accustomed to performing arthroscopy, the learning curve is much steeper: whereas with the single-port technique it takes about fifty cases to achieve a certain level of proficiency, here it takes only ten or fifteen.
This breaks down a barrier and should help popularize the technique and endoscopy in general, along with the patient benefits we’ve mentioned.
The other major advantage is that this technique opens up much broader treatment options. Other spinal surgeries are now possible using this technique, all through very small incisions in a minimally invasive manner.
For us, as a training institution, the fact that the technique takes less time to master and has highly educational aspects—thanks to improved video visualization of the surgical field—is also very valuable and will help make it more widely available more quickly.
How does the postoperative recovery go?
We keep the patient overnight for monitoring to ensure there are no complications. Recovery is faster and involves less pain: with the conventional technique, we often have to administer morphine, whereas here, simple pain relievers are sufficient. Since there is less muscle damage, functional recovery is rapid.
Following this initial success, do you plan to expand the use of this technique?
As I mentioned, this surgical technique can be adapted for several surgical indications, including those involving the cervical or thoracic spine. In South Korea, significant work has been done in this area over the past 15 years, enabling them to widely adopt the practice. From this perspective, I see great potential.
For now, I will obviously seek to continue refining my skills and reserve it initially for primary surgeries before using it on revision surgeries (i.e., reoperations), where other constraints come into play. But I fully intend to expand its use to lumbar disc herniations, and likely later to certain cervical surgeries.
The advantage is that if the technique proves too complex in certain cases, we can easily revert to the conventional microscope technique without any risk to the patient: the procedure therefore remains just as safe even during the refinement phase.
Interview by Yannick Richter, Communications Officer