The cesarean section rate in Switzerland has risen significantly over the past few decades (32.6% in 2020 compared to 22.9% in 1998, according to the Federal Statistical Office).
One of the main reasons is the increase in the number of repeat cesarean sections performed out of fear of uterine rupture, which can occur—albeit rarely—during an attempt at vaginal birth after cesarean (VBAC). Clinical practice guidelines recommend attempting a VBAC when conditions are favorable. It is therefore important to carefully select candidates with a good prognosis for a successful VBAC and a low risk of uterine rupture.
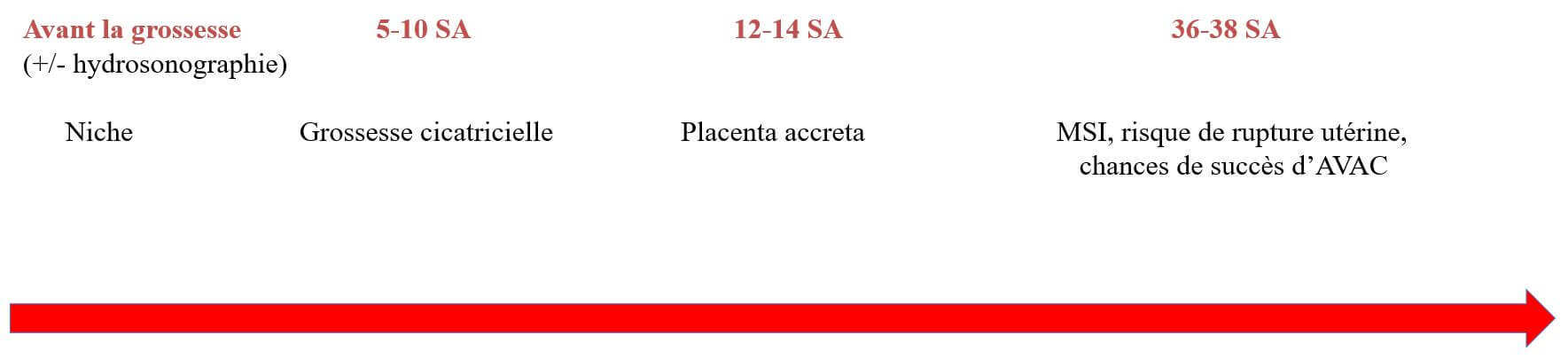
Measuring the lower uterine segment (LUS) by ultrasound between 36 and 38 weeks of gestation has been proposed as a tool for assessing the risk of uterine rupture during delivery. In the prospective study conducted by Rozenberg in 1996, a LUS > 3.5 mm was associated with a reduced risk of uterine injury (defined as uterine ruptures and dehiscences) and had excellent negative predictive value (1). This study was limited by the high incidence (4%) of uterine complications and the absence of transvaginal ultrasound evaluation. In 2010, we demonstrated that an MSI ≤ 2.3 mm could predict the majority of uterine ruptures (2). A systematic review of 12 studies involving a total of 1,834 women confirmed the strong association between the MSI and uterine injuries (3). The main challenge with the MSI stems from the fact that the studies are highly heterogeneous, both in terms of measurement techniques and the threshold value to be considered.
In 2016, we published a prospective multicenter study involving 984 attempts at VBAC and demonstrated that by incorporating the thickness-to-diameter ratio (MSI) into the decision regarding mode of delivery, using a threshold value of 2.5 mm, no symptomatic uterine ruptures occurred (4).
Rozenberg (5) recently published a randomized study involving 2,948 patients, comparing the incidence of maternal-fetal complications (defined by a composite endpoint including uterine rupture) between patients for whom cervical thickness measurement by ultrasound was taken into account in the choice of mode of delivery (MSI group) and those for whom this ultrasound had not been performed (control group). No significant difference was observed between the two groups for the primary outcome measure. However, this study had limitations: first, it lacked sufficient statistical power to demonstrate a significant difference in the incidence of uterine rupture between the two groups studied. There was even a trend toward a reduced risk of uterine rupture in the MSI group (0.4% versus 0.9%, respectively; relative risk: 0.43; 95% confidence interval: 0.15–1.19). Furthermore, MSI was performed exclusively via the abdominal route, whereas the combination of abdominal and endovaginal routes is the method of choice: the abdominal route allows for better visualization of the lower uterine segment (LUS) in cases of uterotomy performed in the upper part of the LUS (e.g., prior cesarean section without labor), whereas endovaginal measurement provides better information in cases of uterine incision made lower down, near the cervix (prior cesarean section during labor) or in cases of obesity (6)
A growing number of authors are also interested in the ultrasound evaluation of the cesarean scar as early as the first trimester of pregnancy. At this stage, it is very important to diagnose an intra-scar pregnancy—a potentially serious complication—and to suspect placenta accreta early in pregnancy (7).
As for the evaluation of the uterine scar in nonpregnant women, it is also of interest, particularly in those presenting with symptoms such as intermenstrual bleeding, pain, and infertility.
Experts have proposed a classification system for these scars (see the cited article) (8).
There is no proven link between the appearance of a cesarean scar and the risk of uterine rupture during the first trimester or in nonpregnant women.
Following Rozenberg’s article, some seem quick to rule out IMR. In our opinion, we must continue to assess it and incorporate it into the discussion with the patient regarding the mode of delivery, weighing the risks and benefits of attempting a VBAC. We believe this is the key to providing care tailored to each woman in labor, thereby enabling a safe attempt at VBAC. We must also continue to evaluate the uterine scar in non-pregnant women, starting in the first trimester, to rule out any potential complications.
Above all, we must continue research in this exciting field.
The MFM Center is actively involved in this field. As part of this effort, starting in October 2022, we will launch a monthly clinic at the Echofemme ultrasound center, intended for all patients—whether pregnant or not—who require a more detailed evaluation of their uterine scar.
When should a cesarean scar be evaluated by ultrasound?
PD Dr. med. Nicole Jastrow Meyer, specialist in maternal-fetal medicine
Dr. Romaine Robyr, specialist in maternal-fetal medicine
References
- Rozenberg et al. Ultrasonographic measurement of lower uterine segment to assess risk of defects of scarred uterus. Lancet, 1996. 347(8997): p. 281-4
- Bujold et al. Prediction of complete uterine rupture by sonographic evaluation of the lower uterine segment. Am J Obstet Gynecol, 2009. 201(3): p. 320 e1-6
- Jastrow, N., et al., Sonographic lower uterine segment thickness and risk of ute- rine scar defect: a systematic review. J Obstet Gynaecol Can, 2010. 32(4): p. 321-7
- Jastrow N et al. Lower uterine segment thickness to prevent uterine rupture and adverse perinatal outcomes: a multicenter prospective study. Am J Obstet Gynecol. 2016Nov;215(5):604.e1-604.e6
- Rozenberg P et al. Evaluation of the usefulness of ultrasound measurement of the lower uterine segment before delivery of women with a prior cesarean delivery: a randomized trial Am J Obstet Gynecol. 2022 Feb;226(2):253.e1-253.e9
- Jastrow et al. Can third-trimester assessment of uterine scar in women with prior cesarean section predict uterine rupture? Ultrasound Obstet Gynecol. 2016 Apr;47(4):410-4.)
- Stirnemann J et al. First-trimester uterine scar assessment by transvaginal ultrasound. Am J Obstet Gynecol, 2011. 205(6): p. 551 e1-6
- Jordans I. et al. Sonographic examination of uterine niche in non-pregnant women: a modified Delphi procedure. Ultrasound Obstet Gynecol. 2019 Jan;53(1):107-115.